How does universal health coverage work?
canadian Medicare — Canada ’ south universal joint, publicly funded health care arrangement — was established through federal legislation in the first place passed in 1957 and in 1966. The Canada Health Act of 1984 replaces and consolidates the two former acts and sets home standards for medically necessity hospital, diagnostic, and doctor services. To be eligible to receive broad federal cash contributions for health care, each peasant and territorial ( P/T ) health insurance plan needs to comply with the five pillars of the Canada Health Act, which stipulate that it be :
- Publicly administered
- Comprehensive in coverage conditions
- Universal
- Portable across provinces
- Accessible (for example, without user fees).
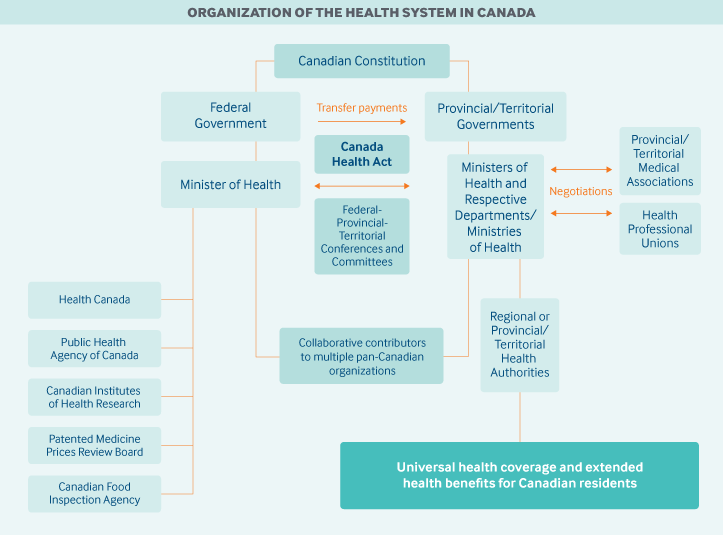
Role of government: canadian P/T governments have chief responsibility for finance, organizing, and delivering health services and supervising providers. The jurisdictions immediately fund physicians and drug programs, and contract with delegate health authorities ( either a individual peasant authority or multiple subprovincial, regional authorities ) to deliver hospital, community, and long-run care, deoxyadenosine monophosphate good as mental and public health services .
The union politics cofinances P/T universal health insurance programs and administers a scope of services for certain populations, including eligible foremost Nations and Inuit peoples, members of the Canadian Armed Forces, veterans, resettled refugees and some refugee claimants, and inmates in federal penitentiaries. It besides regulates the safety and efficacy of checkup devices, pharmaceuticals, and natural health products, funds health inquiry and some data engineering systems, and administers several populace health functions on a national scale.
Reading: Canada
At the national degree, a diverseness of governmental agencies oversee specific functions :
- Health Canada, which is the federal ministry of health, plays a key regulatory role in food and drug safety, medical device and technology review, and the upholding of national standards for universal health coverage.
- The Public Health Agency of Canada is responsible for public health, emergency preparedness and response, infectious and chronic disease control and prevention, and health promotion.
- A new federal government department, Indigenous Services Canada, funds certain health services for First Nations and Inuit.
Most providers are autonomous under P/T police ; they are registered with a provincial regulative body ( such as the College of Physicians and Surgeons ) that ensures that education, train, and quality-of-care standards are met .
Most provinces have an ombudsperson who advocates on behalf of patients .
Role of public health insurance: Total health spend is estimated to have reached 11.5 percentage of GDP in 2017 ; the populace sector and secret sector accounted for approximately 70 percentage and 30 percentage of full health expenditures, respectively.1 Each P/T health indemnity design covers all medically necessary hospital and doctor services ( on a prepay footing ). supplementary services, or those not covered under canadian Medicare, are largely privately financed, either from patient out-of-pocket payments or through employer-based or individual policy .
Provinces and territories cover all of their own residents in accordance with their respective residency requirements.2 Temporary legal visitors, undocumented immigrants, visitors who stay in Canada beyond the duration of a legal permit, and those who enter the area illegally are not covered by any federal or P/T program. Provinces and territories provide limited emergency services to these populations — no doctor or hospital can refuse to provide manage in an emergency, and midwives provide some pregnancy services.3
The independent fund source is general P/T government gross. Most P/T tax income comes from tax. About 24 percentage ( an estimated CAD 37 billion, or USD 29.4 billion, in 2017–2018 ) is provided by the Canada Health Transfer, the federal program that funds health care for provinces and territories.4
Role of private health insurance: Private indemnity, held by about two-thirds of Canadians, covers services excluded under cosmopolitan health coverage, such as vision and alveolar consonant care, outpatient prescription drugs, rehabilitation services, and private hospital rooms. In 2015, approximately 90 percentage of premiums for private health plans were paid through employers, unions, or other organizations under a group condense or uninsured contract ( by which a design sponsor provides benefits to a group outside of an policy contract ). In 2017, private insurance was estimated to account for 12 percentage of total health spend. 5 The majority of insurers are for-profit.6

Services covered: To qualify for federal fiscal contributions, P/T indemnity plans must provide first-dollar coverage of medically necessity doctor, diagnostic, and hospital services ( including inpatient prescription drugs ) for all eligible residents. All P/T governments besides provide public health and prevention services ( including immunizations ) as separate of their public programs .
however, there is no nationally defined statutory benefit package ; most public coverage decisions are made by P/T governments in junction with the checkup profession. Because of this, coverage varies across P/T policy plans for services not federally mandated as medically necessary, including outpatient prescription drugs, mental health care, vision caution, alveolar consonant care, base wish, obstetrics services, medical equipment, and hospice care .
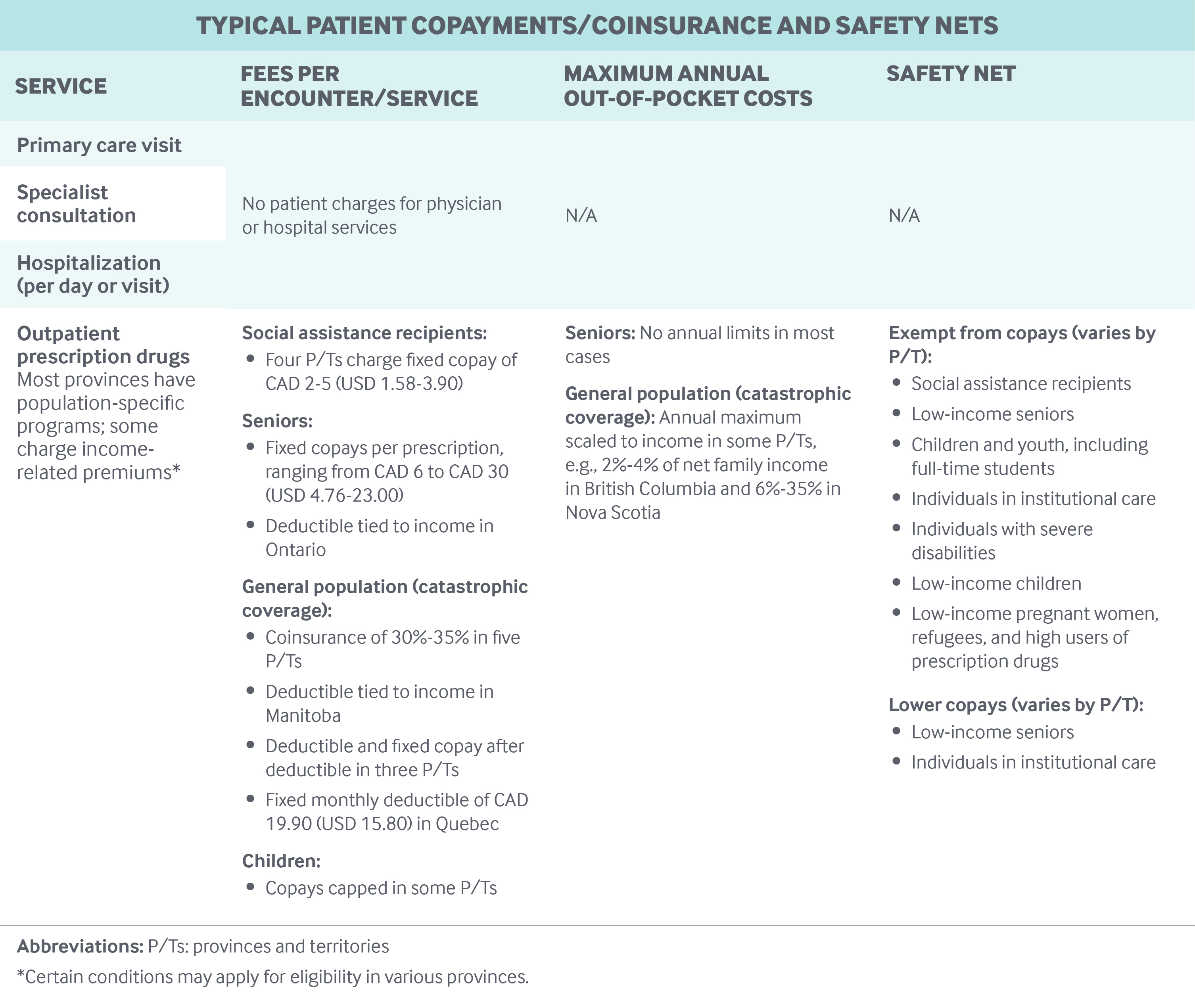
Most provinces have public prescription drug coverage programs for specific populations, such as recipients of social aid, seniors aged 65 and older, and children and youth. Some programs charge premiums, frequently income-related.7
There are some health services that, for the most depart, are not covered by any P/T policy plan, including dental services, physical therapy, psychologist visits, chiropractic caution, and cosmetic or credit card operating room .
Cost-sharing and out-of-pocket spending: There is no cost-sharing for publicly insured doctor, diagnostic, and hospital services. Physicians are not allowed to charge patients prices above the negotiate fee agenda .
In 2016, out-of-pocket payments were estimated to represent about 15 percentage of total health spending ; the majority was spent on nonhospital institutions ( chiefly long-run worry homes ), prescription drugs, alveolar consonant care, and vision care.8
Safety nets: To help cover need prescriptions, provinces and territories provide outpatient drug plans to some individuals lacking individual employer-sponsored indemnity. Most P/T outpatient drug plans operate as payers of last resort, targeting people on social aid or of retirement age. These plans vary well. For case, Quebec administers a universal drug plan by mandating that eligible individuals have private coverage and enrolls those not eligible for private coverage in the public plan. In contrast, Ontario, Canada ’ s most populous province, administers a universal prescription drug drug plan for seniors, children and young person without individual coverage, and recipients of social aid .
P/T governments besides provide some relief for people with high out-of-pocket expenses. After citizens yield more than 3 percentage of their net income, or CAD 2,288 ( USD 1,816 ), whichever is less, for eligible medical expenses per year, they can receive a 15 percentage tax accredit for any remaining expenses.9
In addition, provinces and territories pay for accommodation and food expenses ( beyond nursing care ) of destitute individuals in publicly financed long-run care facilities .
How is the delivery system organized and how are providers paid?
Physician education and workforce : Students who obtained a medical degree from one of Canada ’ s 17 public checkup schools paid an median annual tutelage of CAD 14,780 ( USD 11,730 ) in 2018–2019.10 About 27 percentage of Canada ’ s physicians received their degree outside Canada.11
In 2017, 92 percentage of physicians practiced in urban locations.12 There are no national programs to ensure a provide of doctors in rural and distant locations. however, most provinces have rural practice initiatives. For model, Alberta ’ s Rural, Remote, Northern Program guarantees physicians an income greater than CAD 50,000 ( USD 39,382 ) .13
Primary care: In 2017, there were 2.3 practicing physicians per 1,000 population ; about half ( 1.2 per 1,000 population ) were family physicians, or general practitioners ( GPs ), and the rest specialists ( 1.15 per 1,000 population ) .14 GPs act largely as gatekeepers, and many provinces pay lower fees to specialists for non-referred consultations .
Most physicians are freelance in private practices. In 2014, the end year of the National Physician Survey, about 46 percentage of GPs worked in a group practice, 19 percentage in an interprofessional exercise, and 15 percentage in a solo practice.15 In several provinces, networks of GPs work together and share resources, with variations across provinces in the composition and size of teams.16
In 2017, about 62 percentage of determine nurses ( register nurses, nurse practitioners, and licensed virtual nurses ) worked in hospitals and 15 percentage in community health settings on salaries.17 In the three northern territories ( Yukon, Northwest Territories, and Nunavut ), elementary wish is much nurse-led .
In theory, patients have complimentary option of a GP ; in practice, however, patients may not be accepted into a doctor ’ randomness practice if the doctor has a close up number. The requirements for affected role registration vary well by state and territory, but no legal power has implemented stern rostering.18 Quebec, through Family Medicine Groups, has used patient registration and added ( human and fiscal ) resources to improve entree to care .
Fee-for-service is the primary coil imprint of doctor requital, although there has been a motion toward alternate forms of requital, such as capitation. In 2016–2017, fee-for-service payments made up about 45 percentage of GP payments in Ontario, 72 percentage in Quebec, and 82 percentage in British Columbia ; capitation and, to a lesser extent, salaries made up remaining payments.19
In 2016–2017, the average clinical payment was CAD 276,761 ( USD 219,651 ) for family medicine, CAD 357,264 ( USD 283,543 ) for aesculapian specialties, and CAD 477,406 ( USD 378,894 ) for surgical specialties.20 In most provinces, specialists have the lapp fee schedule as primary care physicians .
peasant ministries of health negotiate doctor fee schedules ( for primary and specialist care ) with medical associations. In some provinces, such as british Columbia and Ontario, payment incentives have been linked to performance .
Outpatient specialist care: Specialists are largely freelance. There are few formal multispecialty clinics .
The majority of specialist care is provided in hospitals, on both an inpatient and an outpatient footing, although there is a drift toward providing less-complex services in nonhospital diagnostic or surgical facilities .
Specialists are paid by and large on a fee-for-service footing, although there is variation across provinces. For example, in Quebec, alternate payment structures made up about 15 percentage of sum payments to specialists in 2016–2017, as compared to 22 percentage in British Columbia and 33 percentage in Saskatchewan .
Patients can choose to go immediately to a specialist, but it is more common for GPs to refer patients to specialty care. Specialists who bill P/T populace insurance plans are not permitted to receive payment from privately insured patients for services that would be covered under public insurance .
Administrative mechanisms for direct patient payments to providers: The majority of physicians and specialists bill P/T governments immediately, although some are paid a wage by a hospital or facility. Patients may be required to pay out-of-pocket for services that are not covered by populace policy plans .
After-hours care: After-hours manage is often provided in physician-led walk-in clinics and hospital hand brake rooms. In most provinces and territories, a exempt call service allows citizens to get health advice from a register nurse 24 hours a day.
Read more: A Man Quotes Maritime Law To Avoid Ticket
historically, GPs have not been required to provide after-hours care, although newer group-practice arrangements stipulate requirements or fiscal incentives for providing after-hours care to registered patients.21 In 2015, 48 percentage of GPs in Canada ( 67 % in Ontario ) reported having arrangements for patients to see a sophisticate or nurse after hours.22 even, in 2016, only 34 percentage of patients reported having access to after-hours worry through their GP.23
Hospitals: Hospitals are a mix of populace and private, predominantly nonprofit organization, organizations. They are much managed by delegate health authorities or hospital boards representing the residential district. In most provinces and territories, many hospitals are publicly owned,24 whereas in Ontario they are predominantly private nonprofit organization corporations.25
There are no specific data on the number of private for-profit clinics ( chiefly diagnostic and surgical ). however, a 2017 survey identified 136 private for-profit clinics across Canada.26
Hospitals in Canada by and large operate under annual global budgets, negotiated with the provincial ministry of health or delegated health authority. however, several provinces, including Ontario, Alberta, and British Columbia, have considered inaugurate activity-based fund for hospitals, paying a sterilize amount for some services provided to patients.27
Hospital-based physicians generally are not hospital employees and are paid fee-for-service directly by the provincial ministries of health .
Mental health care: Physician-provided mental health care is covered under canadian Medicare, in addition to a break up system of allied services. Hospital-based genial health worry is provided in specialization psychiatric hospitals and in general hospitals with mental health beds. The P/T governments all provide a rate of community mental health and addiction services, including event management, help for families and caregivers, community-based crisis services, and supportive housing.28
private psychologists are paid out-of-pocket or through secret insurance. Psychologists who work in publicly funded organizations receive a wage .
Mental health has not been formally integrated into primary care. however, some organizations and provinces have launched efforts to coordinate or collocate mental health services with primary coil care. For example, in Ontario, an intersectoral mental health strategy has been in place since 2011 and was expanded in 2014 to better integrate genial health and primary care.29
Long-term care and social supports: Long-term concern and end-of-life manage provided in nonhospital facilities and in the community are not considered guarantee services under the Canada Health Act. All P/T governments fund such services through general tax, but coverage varies across jurisdictions. All provinces provide some residential caution and some combination of sheath management and nursing care for home care clients, but there is considerable variation when it comes to other services, including medical equipment, supplies, and home support. many jurisdictions require copayments .
eligibility for home and residential long-run care services is by and large determined via a indigence judgment based on health status and functional impairment. Some jurisdictions besides include means-testing. About half of P/T governments provide some family care without means-testing, but access may depend both on assessed priority and on the handiness of services within capped budgets.30
The government funds personal and nursing care in residential long-run facilities. In addition, fiscal supplements based on ability to pay can help support room-and-board costs. Some provinces have established minimum residency periods as an eligibility condition for adeptness admission .
Spending on nonhospital institutions, most of which are residential long-run caution facilities, was estimated to account for barely over 11 percentage of total health expenditures in 2017, with finance by and large from public sources ( 70 % ) .31 A roughly equal mix of private for-profit, private nonprofit organization, and public facilities provide facility-based long-run care .
Public fund of home wish is provided either through P/T government contracts with agencies that deliver services or through government stipends to patients to purchase their own services. For example, British Columbia ’ s Support for Independent Living plan allows clients to purchase their own home-support services.32
Provinces and territories are responsible for delivering palliative and end-of-life care in hospitals ( covered under Canadian Medicare ), where the majority of such costs occur. But many provide some coverage for services outside those settings, such as doctor and breastfeed services and drug coverage in hospices, in nurse facilities, and at home .
In June 2016, the union government introduced legislation that amended the condemnable code to allow eligible adults to request aesculapian aid in dying from a doctor or nurse practitioner. Since that meter, P/T governments and checkup associations have set up processes and regulative frameworks to allow for checkup aid in dying for individuals facing terminal or irreversible illnesses .
More than 8 million Canadians are estimated to have provided amateur support to persons living with chronic health and social needs in 2012.33 accompaniment for informal caregivers ( estimated to provide 66 % to 84 % of care to the aged ) varies by province and territory.34 For example, Nova Scotia ‘s Caregiver Benefit Program offers eligible caregivers and care recipients CAD 400 ( USD 317 ) per month.35 There are besides some federal programs, including the Canada Caregiver Credit and the Employment Insurance Compassionate Care Benefit .
What are the major strategies to ensure quality of care?
many provinces have agencies responsible for producing health care arrangement reports and for monitoring organization performance. In addition, the Canadian Institute for Health Information produces regular public reports on health system performance, including indicators of hospital and long-run care facility performance. To date, there is no information publicly available on doctors ’ performance across the nation. Most provinces post drumhead inspection reports on-line .
Home care agencies do not have report standards similar to those for residential long-run manage. The canadian Institute for Health Information has the Home Care Reporting System, which contains demographic, clinical, running, and resource utilization data for clients served by publicly funded programs across Canada. however, in 2018, only eight jurisdictions were submitting data.36
The function of fiscal incentives to improve quality is limited. At the doctor floor, they have had, to date, little demonstrable effect on quality.37 Professional revalidation requirements for physicians, including those for continuing education and peer review, vary across provinces .
A diverseness of other choice initiatives are in build up :
- The federally funded Canadian Patient Safety Institute promotes best practices and develops strategies, standards, and tools.
- Provincial quality councils facilitate process improvements to produce higher-quality health care.
- The Optimal Use Projects program, operated by the Canadian Agency for Drugs and Technologies in Health, provides recommendations (though not formal clinical guidelines) to providers and consumers to encourage the appropriate prescribing, purchasing, and use of medications.
- The federally funded Canadian Foundation for Healthcare Improvement works with P/T governments to implement performance improvement initiatives.
- Accreditation Canada — a nongovernmental organization — provides voluntary accreditation services to about 1,200 health care organizations across Canada, including regional health authorities, hospitals, long-term care facilities, and community organizations.
- Provincial cancer registries feed data to the Canadian Cancer Registry, a national administrative survey that tracks cancer incidence.
- There is no national patient survey, although a standardized acute-care hospital inpatient survey developed by the Canadian Institute for Health Information has been implemented in several provinces. Each province has its own strategies and programs to address chronic disease.
- The P/T premiers, or prime ministers, established the Health Care Innovation Work Group in 2012 to improve quality by, for example, promoting guidelines for treating heart disease and diabetes and reducing costs.
What is being done to reduce disparities?
The Public Health Agency of Canada includes health disparities reporting in its mandate, and the Canadian Institute for Health Information besides reports on disparities in health care and health outcomes, with a concenter on lower-income Canadians.38 No courtly or periodic process exists to measure disparities ; however, several P/T governments have departments and agencies devoted to addressing population health and health inequities .
Health disparities between autochthonal and nonindigenous Canadians are a concern for politics at both the federal and the P/T level. The 2018 federal budget offers new financing of CAD 5 billion ( USD 3.9 billion ) for autochthonal people, building on previous investments totaling CAD 11.8 billion ( USD 9.3 billion ). The money is earmarked for education, the environment ( for exercise, water quality ), and health and social services.39
In 2015, the Truth and Reconciliation Commission, which was established to collect stories regarding the events and effects of the indian Residential School bequest, released a series of calls to action, including respective addressing health disparities that affect autochthonal communities.40
In Ontario, a scheme to improve the health of autochthonal people was launched in 2016, with emphasis on investments in primary coil care, cultural competence training for health care providers, access to fresh yield and vegetables, and mental health services for first Nations youth.41
What is being done to promote delivery system integration and care coordination?
Provinces and territories have introduced respective initiatives to improve the integration and coordination of manage for chronically ill patients with building complex needs. These include Divisions of Family Practice ( British Columbia ), family Medicine Groups ( Quebec ), the Regulated Health Professions Network ( Nova Scotia ), and Health Links ( Ontario ) .
In addition, Ontario has long-standing community-based and multidisciplinary primary manage models in place, including Community Health Centres and Aboriginal Health Access Centres. Ontario besides continues to expand a pilot program program that bundles payments across different providers. This alternative payment border on is expected to improve concern coordination for patients as they transition from hospital to the community.42
What is the status of electronic health records?
Uptake of health information technologies has been slowly increasing in late years. Provinces and territories are responsible for developing their own electronic information systems, with national fund and hold through Canada Health Infoway. however, there is no national strategy for implementing electronic health records and no national patient identifier .
According to Canada Health Infoway, provinces have systems for collecting data electronically for the majority of their populations ; however, interoperability is limited. In 2017, 85 percentage of GPs reported using electronic aesculapian records, but patients have limited access to their own electronic health information.43
How are costs contained?
Costs are controlled chiefly through single-payer buying, and increases in very spend chiefly reflect government investment decisions or budgetary overruns. Cost-control measures include :
- Mandatory global budgets for hospitals and regional health authorities
- Negotiated fee schedules for providers
- Drug formularies for provincial drug plans
- Resource restrictions for physicians and nurses (such as provincial quotas for students admitted annually)
- Restrictions on new investment in capital and technology.
The canadian Agency for Drugs and Technologies in Health oversees the home health technology appraisal summons, which is one mechanism for containing new engineering costs. This agency produces data about thyroxine clinical potency, cost-effectiveness, and broader impact of drugs, medical technologies, and health systems. The means ’ randomness Common Drug Review assesses the clinical potency and cost-effectiveness of drugs and provides coarse, nonbinding formulary recommendations to the publicly funded peasant drug plans ( except in Quebec ) to support greater consistency in access and evidence-based resource allotment .
The federal Patented Medicine Prices Review Board, an mugwump, quasi-judicial soundbox, regulates the introductory prices of fresh patent medications. The board regulates factory gate prices but does not have legal power over wholesale or pharmacy prices, or over pharmacists ’ professional fees .
Since 2010, the Pan-Canadian pharmaceutical Alliance has negotiated lower prices for 95 brand-name medications and has set monetary value limits at 18 percentage of equivalent brand-name drug prices for the 15 most common generics.44 Notwithstanding this pan-Canadian collaboration, jurisdiction over prices of generics and control over pricing and purchasing under public drug plans ( and, in some cases, pricing under private plans ) are held by provinces, leading to some interprovincial version.
In addition, the Choosing Wisely Canada political campaign provides recommendations to governments, providers, and the public on reducing low-value care.45
What major innovations and reforms have recently been introduced?
As noted above, prescription drugs, outside of hospitals, are not universally covered. At the federal level, there are signs of renewed matter to in a pan-Canadian system of drug coverage. In 2018, the Advisory Council on the Implementation of National Pharmacare was established, and an interim report was produced in 2019.46 If a home platform moves fore, it will be the biggest expansion of public financing and coverage since Canadian Medicare was introduced .
Provinces and territories continue to implement structural reforms to improve efficiency. The latest example occurred in 2017 when Saskatchewan replaced its 12 regional health authorities with a single peasant health authority. This first step reflects a national tendency toward greater administrative centralization. similarly, as partially of an evolving reform effort, Manitoba established a one provincial arrangement — Shared Health — to centralize some clinical and administrative services. In 2019, the Ontario government announced its plans to consolidate respective peasant arm ’ s-length agencies, along with the 14 subprovincial health authorities — local Health Integration Networks — that administer and deliver health care for their local anesthetic populations, into a single provincial agency.47






